Featured In

In some women normal breast development is impaired because of a congenital defect. At times this defect involves the chest muscles as well. There are a variety of congenital breast deformities including tuberous/tubular breasts, Poland Syndrome, and asymmetry (different size and/or shape of the breasts).
Many breast deformities are the result of internal scar tissue that contracts and distorts the breast and tissue around it. The tubular breast is the result of a congenital band around the base of the breast.
We are able to correct and perfect your breasts using the 4 different techniques we have developed, BRAVA, Rigottomy, PALF, and RAFT followed by our minimally invasive fat grafting procedure.
Just as in breast augmentation, the chest wall is prepared with the BRAVA device, and fat is grafted like a sculptor would apply clay, modeling the breast with the goal of creating a breast in harmony with the patient’s wishes and the size and shape of the rest of her chest. The deformity is corrected without any incisions, sutures, or scarring.
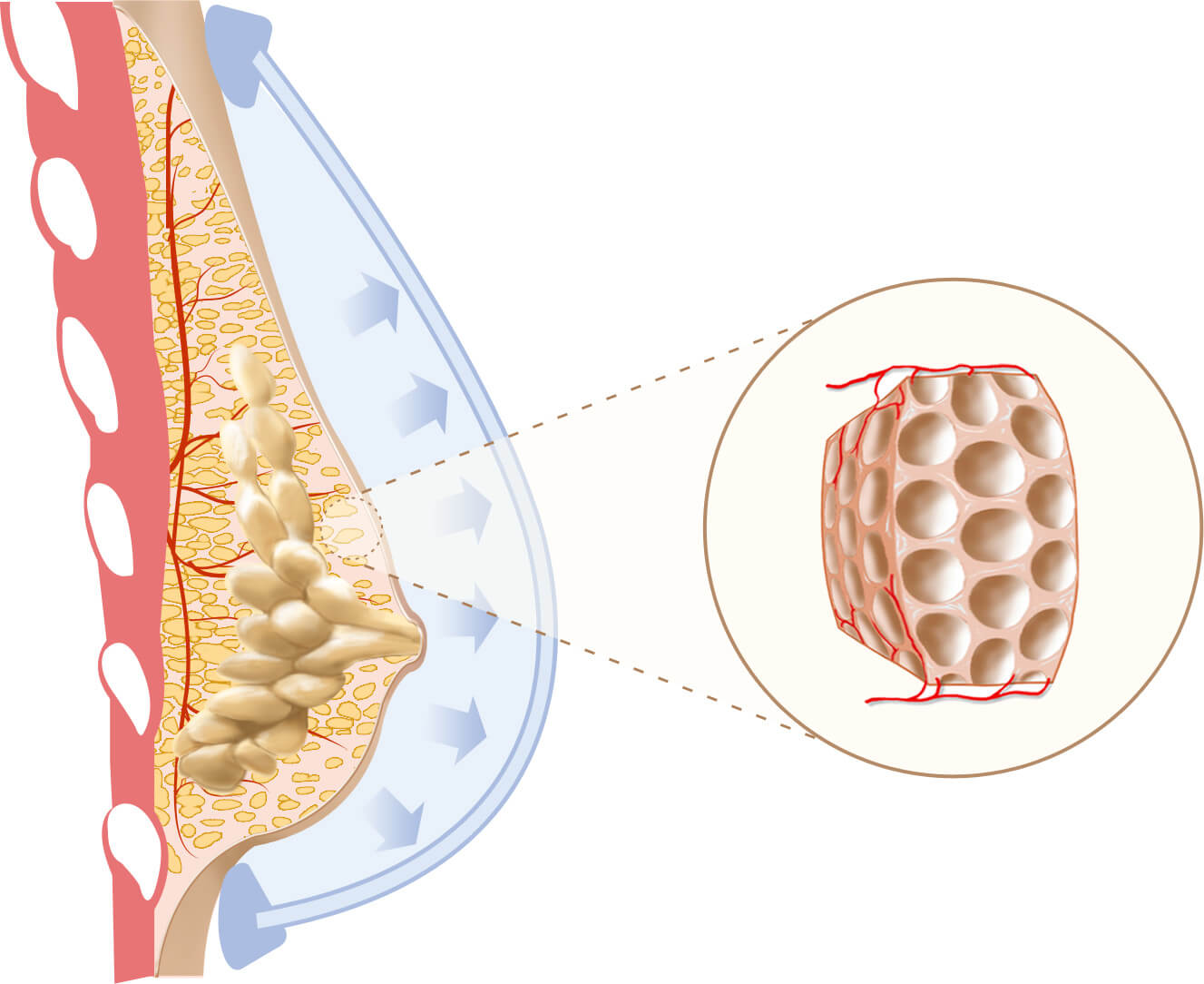
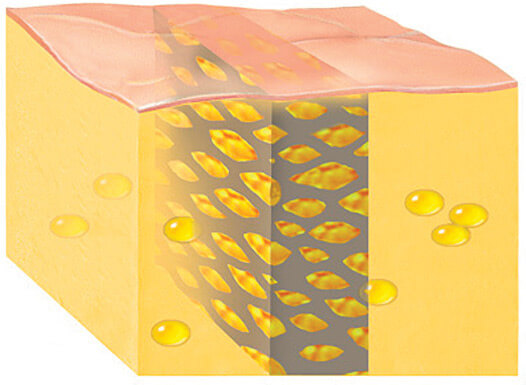
BRAVA system is placed over the breast area when you sleep. Patients with tubular, asymmetry or other breast deformity wear the BRAVA before the surgery. Vacuum inside the domes pulls the breast tissue outward to start expansion. Inset shows loosening of the normal tissue density. It’s the key for a high rate of fat survival.
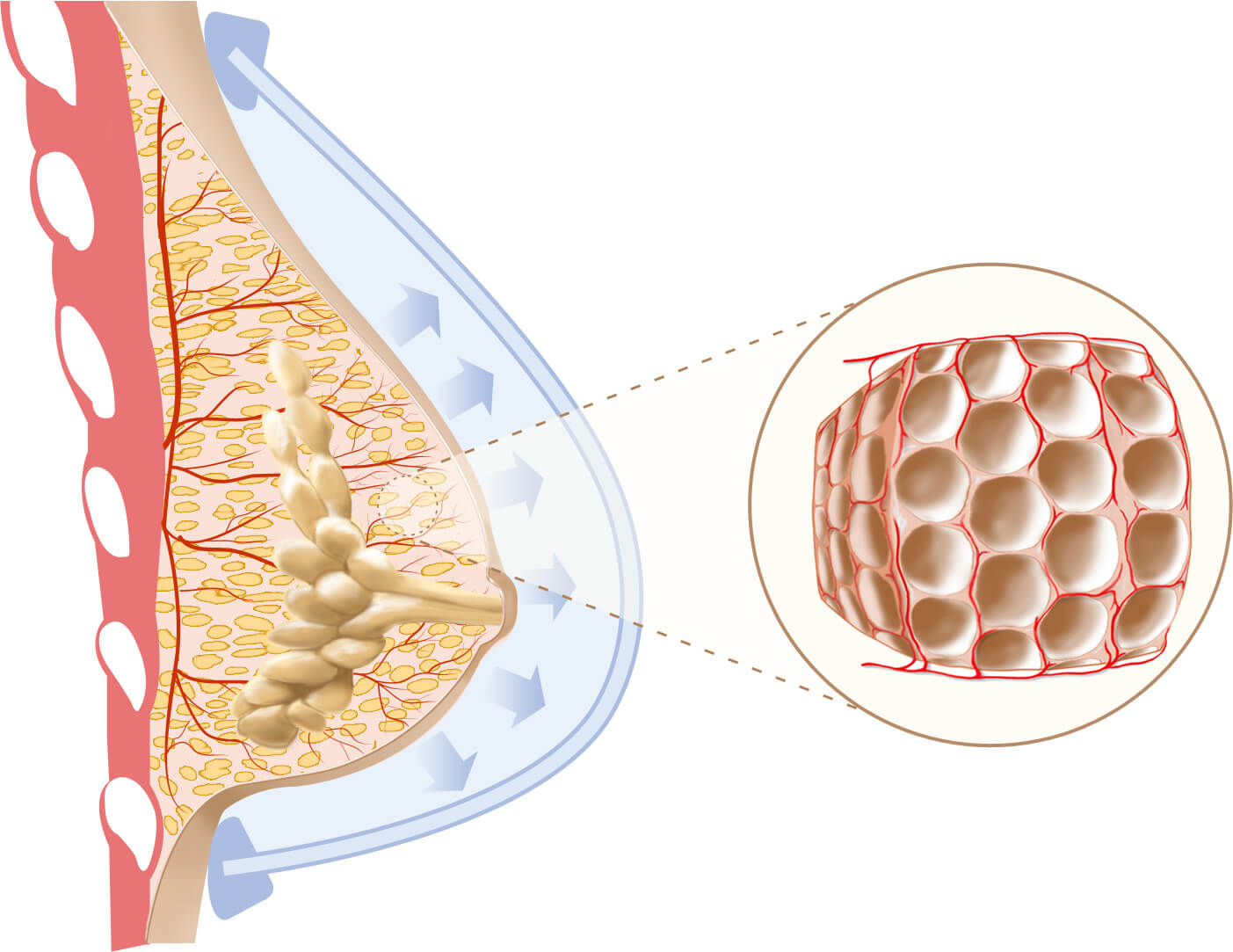
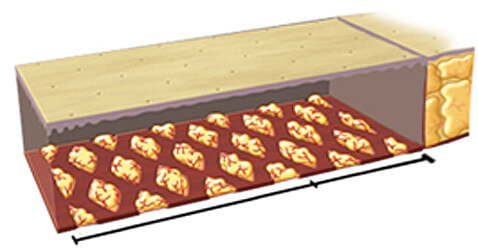
With continued expansion, the breast enlarges even more. It begins to loosen and release scar or constricted tissue causing the deformity. Inset shows the loosening up of the tissues as they open up like an expanding sponge to make room for the grafts. Notice that with this rapid expansion there aren’t any new fat cells, only a loosening of the normal tissue density with stretched out fibers and tiny new blood capillaries along the expanded structure ready to accept the grafts.
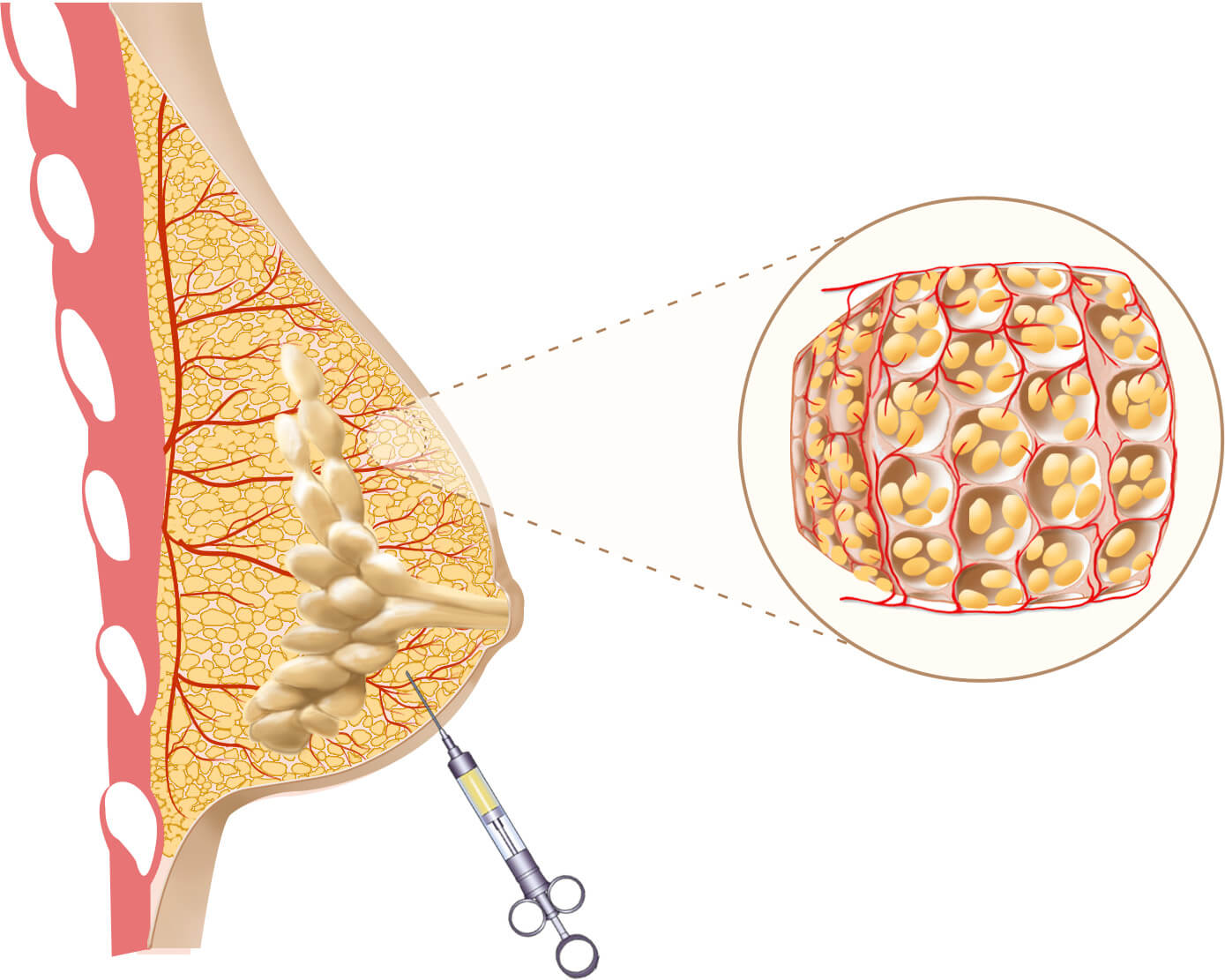
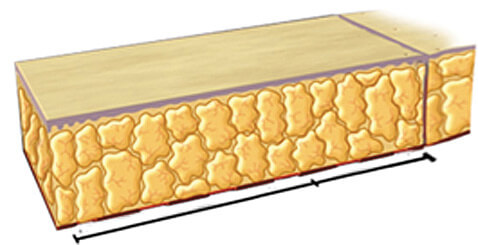
The expanded space is grafted with fat harvested from your desired body area. No cuts or incisions are made, only needle pokes. The fat fills up the expanded vascular structure and restores the normal cellular density. Inset shows how new blood vessels help keep the fat deposits alive. The breast has been augmented with tissue engineered fat.
In cases with deforming, tight, scar tissues, there is not any room for a fat graft. Therefore the scar needs to be broken up or removed. If we excise the scar (internal scar tissue), we leave a large empty space that will not support a fat graft. Instead, we loosen the scar by puncturing it with multiple passages of a fine needle.
The tiny spaces left behind after the needle nicks become sites for the placement of the grafts. We call this technique Rigottomy after Dr. Gino Rigotti who first introduced it to us.
The Rigottomy has served as an excellent way to manage the deforming scar. It allows us to loosen up a cicatrix (scar) and convert it into a larger matrix (scaffold for receiving a fat graft).
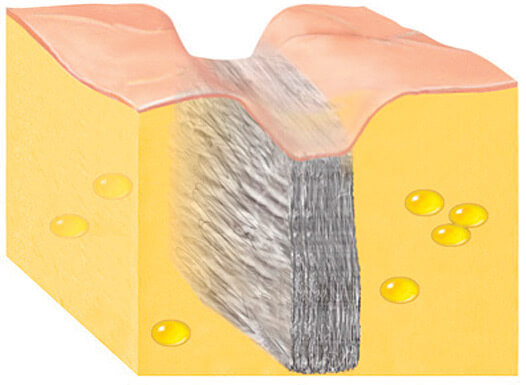
A scar can be likened to a rock-hard brick wall separating two gel-like normal fat compartments. The scar is typically tight and often tethers down the skin.
To graft that hard scar with fat we need to loosen it and open in it tiny interstices where the fat droplets can lodge and survive. We do it without any incisions through the skin, using fine needles that repeatedly nick the scar until it loosens up. Once the scar is no longer tight, it becomes like a scaffold matrix that we fill with fat droplets that will stretch and expand it until it no longer tethers down the skin. Of even greater importance, as it fills up with fat, the scar softens to become more like the tissues around it. Repeating the process will completely melt away the cicatrix and replace it with normal fat.
We use the PALF when the scar is restricting the advancement of the tissue and is tightly tethering the skin. It is used mostly to overcome skin shortage. It is based upon the same principle as the Rigottomy, but in this application we preferentially nick the scar such as it will mesh expand in the direction of skin deficiency in order to further advance the tissues in that direction. In technical terms, the PALF is the two-dimensional application of the three-dimensional Rigottomy.
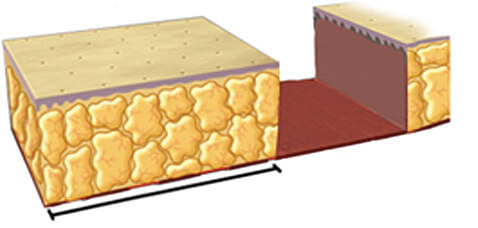
Tissue deficit skin gap that cannot be closed even after maximally stretching the surrounding normal skin and subcutaneous fat.
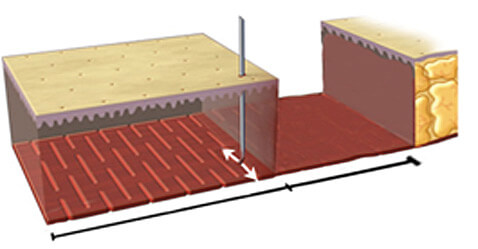
Multiple needle punctures through the skin nick the deeper tissues (whether scar or tight fascia) that restrict the skin advancement to create a pattern of tiny alternating slits (Percutaneous Aponeurotomy).
The generated mesh pattern is expanded, loosening the restriction and allowing the overlying skin to advance and treat the defect without tension.
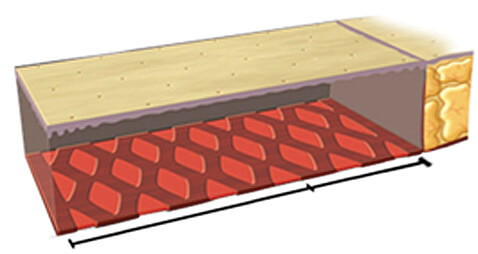
The tiny spaces left behind by the opening of the expanded mesh are filled with fat micrografts (Lipo-Filling).
Regenerated tissue fills up the original tissue deficit as the fat graft matures and the skin tension dissipates.
The RAFT enables us to advance a significant amount of abdominal tissue into the breast. With the RAFT we slide up the lax abdominal tissue into the breast without any incision. This is like an abdominoplasty (tummy tuck) in reverse as we pull the tissues up instead of down like we would in the standard abdominoplasty. Using only needle puncture nicks, the PALF maneuver allows us to advance the abdominal tissue into the breast without having to cut it out and transfer it as a flap. The tissue brought up from the abdomen serves to provide the skin envelope needed to better contour the breast and to better define the inframammary breast fold. It is also an additional recipient matrix for fat grafting that can provide more volume and help fill contracted areas.
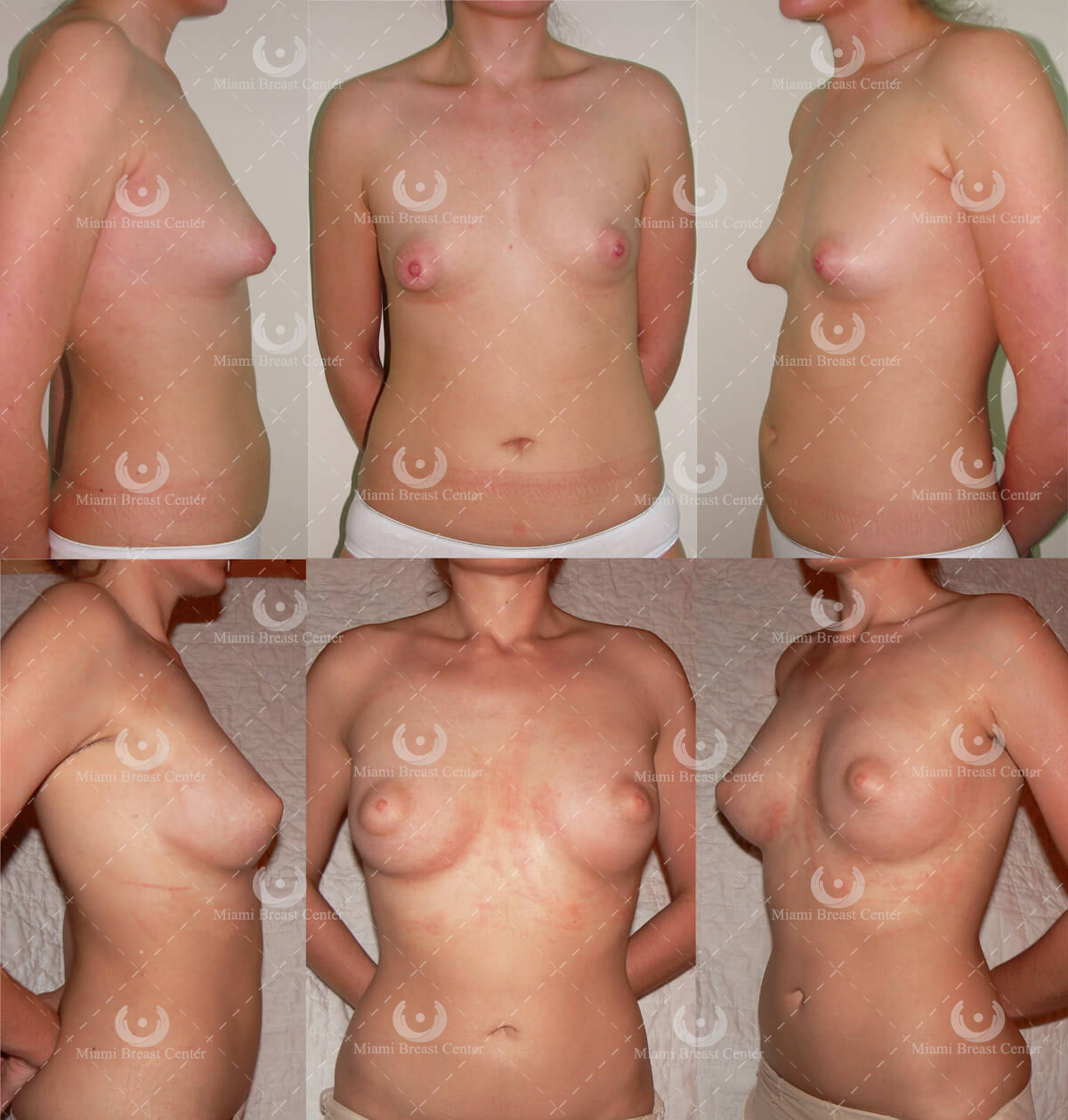
A young woman with tubular breast deformity. To correct the tuberous deformity, she underwent the BRAVA expansion, so the breast enlarges and begins to loosen the congenital constriction and increases the circulation in this area. Using the Rigottomy technique, the scar is loosened and converted into a recipient area for the fat grafts. The PALF method is also used to generate a normal breast fold, shape and form.
The results are natural and fuller breasts with normal appearance. Her results are stable at six months post operation. These results are achieved with BRAVA expansion, fat transfers and fine needle sticks.
See More PhotosThese breast conditions result from a developmental deformity of the breast in which an internal constriction band across the base of the breast, primarily in its lower portion, prevents it from developing fully over the entire surface of the chest. The growth is stunted and remains limited to the area around the nipple. The magnitude of the deformity varies. In a mild form there is a higher inframammary fold and a shorter distance from the lower edge of the nipple area to the fold of the breast on the chest wall (inframammary fold). As the severity of the deformity advances, the lower portion of the breast is less prominent and eventually, in severe cases, totally absent, with the appearance of the breast being one of a tube with a puffy, nipple areola complex at the end.
Tuberous breasts are not simply small or underdeveloped breasts. There is a specific look of the deformity which can range from mild (constricted breasts with a tight base or high fold) to severe (breasts that look like a tube). Typical characteristics include:
Treatment of this deformity involves all the techniques mentioned previously: BRAVA, PALF, and RAFT. We bring down the infamammary fold, do some sculptural fat grafting, and conclude with the support of the BRAVA for several weeks.

Poland Syndrome is a congenital deformity of the chest which can vary from a significant absence of breast tissue to an extreme situation where there is not any breast tissue or pectoral muscle. Treatment is the same as in tuberous breast: BRAVA +AFT (Autologous Fat Transfer) with the PALF and RAFT as needed.
Asymmetry of the breasts is a deformity occurring when the breasts are two different sizes or shapes. Asymmetry issues also occur with sagging or drooping breasts. Traditional techniques involve the insertion of an implant in the smaller side, a solution that is complication-prone and rarely gets the implant augmented breast to match the other natural side. Most women then end up spending the rest of their lives replacing implants, lifting the droopy normal side to match the implant side, and subjecting themselves to multiple scar-inducing operations.
Sagging, or drooping, happens naturally after menopause, although some patients have this condition due to a congenital deformity. Sagging happens when the suspensory ligaments of the breast (Cooper’s ligaments) loosen up and their ability to support the breast weakens.
BRAVA + AFT allows us to correct the difference in size or asymmetry with the use of our external expander followed by fat transfer to the appropriate breast. In many instances the asymmetry of the breast is a reflection of asymmetry of the entire chest bony structure. Many women don’t recognize this relationship. The situation can be improved but the thoracic cage (bony chest wall) will remain asymmetrical.
Give us a call if you would rather speak with a person, we will be more than happy to help.
(305) 365-5595We will gladly answer any question you may have over email. Click below to get started.
Ask a Question